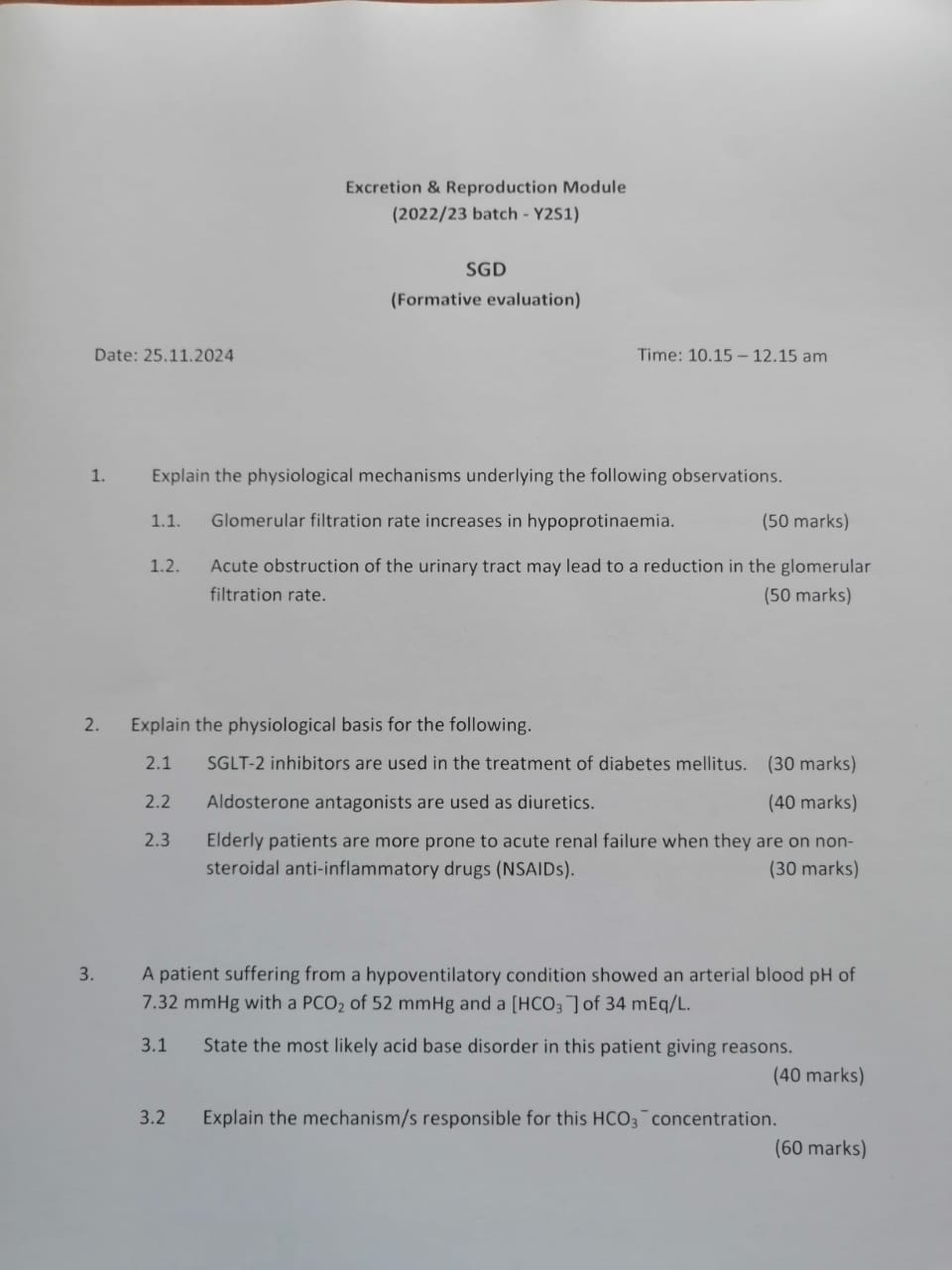
1. Explain the physiological mechanisms underlying the following observations. 1.1. Glomerular filtration rate increases in hypoproteinaemia. 1.2. Acute obstruction of the urinary... 1. Explain the physiological mechanisms underlying the following observations. 1.1. Glomerular filtration rate increases in hypoproteinaemia. 1.2. Acute obstruction of the urinary tract may lead to a reduction in the glomerular filtration rate. 2. Explain the physiological basis for the following. 2.1. SGLT-2 inhibitors are used in the treatment of diabetes mellitus. 2.2. Aldosterone antagonists are used as diuretics. 2.3. Elderly patients are more prone to acute renal failure when they are on non-steroidal anti-inflammatory drugs (NSAIDs). 3. A patient suffering from a hypoventilatory condition showed an arterial blood pH of 7.32 mmHg with a PCO2 of 52 mmHg and a [HCO3-] of 34 mEq/L. 3.1. State the most likely acid-base disorder in this patient giving reasons. 3.2. Explain the mechanism/s responsible for this HCO3- concentration.
Understand the Problem
The question requires explanations of physiological mechanisms related to various medical conditions and treatments, as well as the identification of an acid-base disorder in a clinical scenario.
Answer
1.1. Increased GFR in hypoproteinaemia. 1.2. Decreased GFR in urinary obstruction. 2.1. SGLT-2 inhibitors control glucose. 2.2. Aldosterone antagonists increase urination. 2.3. NSAIDs increase renal risk. 3.1. Compensated respiratory acidosis. 3.2. Increased bicarbonate reabsorption.
1.1. In hypoproteinaemia, there's reduced oncotic pressure in the blood, which decreases the resistance to filtration, thus increasing the glomerular filtration rate (GFR). 1.2. Acute urinary tract obstruction increases tubular pressure, which opposes the filtration pressure, thereby reducing GFR.
2.1. SGLT-2 inhibitors reduce glucose reabsorption in kidneys, aiding glucose control in diabetes. 2.2. Aldosterone antagonists prevent sodium reabsorption in the kidneys, increasing urine output as diuretics. 2.3. NSAIDs reduce renal perfusion by inhibiting prostaglandins, increasing acute renal failure risk in elderly.
3.1. The patient has compensated respiratory acidosis due to high PCO2 and elevated HCO3-. 3.2. The kidneys increase bicarbonate reabsorption to compensate for respiratory acidosis.
Answer for screen readers
1.1. In hypoproteinaemia, there's reduced oncotic pressure in the blood, which decreases the resistance to filtration, thus increasing the glomerular filtration rate (GFR). 1.2. Acute urinary tract obstruction increases tubular pressure, which opposes the filtration pressure, thereby reducing GFR.
2.1. SGLT-2 inhibitors reduce glucose reabsorption in kidneys, aiding glucose control in diabetes. 2.2. Aldosterone antagonists prevent sodium reabsorption in the kidneys, increasing urine output as diuretics. 2.3. NSAIDs reduce renal perfusion by inhibiting prostaglandins, increasing acute renal failure risk in elderly.
3.1. The patient has compensated respiratory acidosis due to high PCO2 and elevated HCO3-. 3.2. The kidneys increase bicarbonate reabsorption to compensate for respiratory acidosis.
More Information
Hypoproteinaemia reduces oncotic pressure, while urinary obstruction increases tubular pressure. SGLT-2 inhibitors lower blood sugar by preventing glucose reabsorption. Aldosterone antagonists act as diuretics by affecting sodium and water retention. NSAIDs can reduce renal perfusion, particularly in vulnerable elderly patients.
Tips
A common mistake is confusing the roles of different diuretics. Understand the hormonal regulation and kidney function impact.
AI-generated content may contain errors. Please verify critical information