Podcast
Questions and Answers
Which of the following is NOT a function of the cell membrane?
Which of the following is NOT a function of the cell membrane?
- To regulate the movement of substances in and out of the cell
- To produce energy for the cell (correct)
- To provide structural support and shape to the cell
- To act as a barrier between the cell and its environment
What is the primary mechanism by which water moves across cell membranes?
What is the primary mechanism by which water moves across cell membranes?
- Active transport
- Passive diffusion (correct)
- Exocytosis
- Endocytosis
Which of the following is NOT a type of active transport?
Which of the following is NOT a type of active transport?
- Endocytosis
- Facilitated diffusion (correct)
- Sodium-potassium pump
- Proton pump
What is the difference between intracellular and extracellular fluid?
What is the difference between intracellular and extracellular fluid?
Why is it important to maintain proper fluid and electrolyte balance?
Why is it important to maintain proper fluid and electrolyte balance?
Which of the following is NOT a primary function of the kidneys related to fluid balance?
Which of the following is NOT a primary function of the kidneys related to fluid balance?
Which of the following statements is TRUE regarding the distribution of electrolytes in the body?
Which of the following statements is TRUE regarding the distribution of electrolytes in the body?
What is the primary mechanism that distributes extracellular fluid (ECF) between the vascular and interstitial compartments?
What is the primary mechanism that distributes extracellular fluid (ECF) between the vascular and interstitial compartments?
Which of the following is a TRUE statement regarding osmolarity/osmolality?
Which of the following is a TRUE statement regarding osmolarity/osmolality?
Which of the following hormones is primarily responsible for moving calcium out of bone?
Which of the following hormones is primarily responsible for moving calcium out of bone?
What is the primary route of fluid intake in the body?
What is the primary route of fluid intake in the body?
Which of the following is an example of a mandatory fluid output route?
Which of the following is an example of a mandatory fluid output route?
What are the two primary hormones involved in regulating renal fluid output?
What are the two primary hormones involved in regulating renal fluid output?
What is the primary driver of thirst?
What is the primary driver of thirst?
What is the typical range for normal serum osmolality?
What is the typical range for normal serum osmolality?
Which of the following conditions is characterized by a decrease in serum osmolality?
Which of the following conditions is characterized by a decrease in serum osmolality?
Which of the following conditions is most likely to cause hypernatremia?
Which of the following conditions is most likely to cause hypernatremia?
Which of the following is an example of an isotonic fluid?
Which of the following is an example of an isotonic fluid?
Which of the following forces promotes fluid movement from the capillaries into the interstitial space?
Which of the following forces promotes fluid movement from the capillaries into the interstitial space?
Which of the following factors contributes to edema by decreasing capillary colloidal osmotic pressure?
Which of the following factors contributes to edema by decreasing capillary colloidal osmotic pressure?
Which of the following forces opposes the movement of fluid from capillaries into the interstitial space?
Which of the following forces opposes the movement of fluid from capillaries into the interstitial space?
Which of these conditions can lead to a decreased urine output?
Which of these conditions can lead to a decreased urine output?
Which of these conditions is NOT a factor leading to increased capillary filtration pressure?
Which of these conditions is NOT a factor leading to increased capillary filtration pressure?
Which of the conditions listed causes an increase in serum osmolality?
Which of the conditions listed causes an increase in serum osmolality?
What type of fluid is necessary to treat dehydration caused by hypernatremia?
What type of fluid is necessary to treat dehydration caused by hypernatremia?
Which of these is a primary mechanism of thirst?
Which of these is a primary mechanism of thirst?
What is the primary role of the renin-angiotensin-aldosterone system (RAAS)?
What is the primary role of the renin-angiotensin-aldosterone system (RAAS)?
How does the sympathetic nervous system contribute to sodium balance?
How does the sympathetic nervous system contribute to sodium balance?
Which of these statements about fluid volume excess is correct?
Which of these statements about fluid volume excess is correct?
Regarding the relationship between body water and age, which of these statements is true?
Regarding the relationship between body water and age, which of these statements is true?
What is the primary cause of intracellular thirst?
What is the primary cause of intracellular thirst?
Which of the following is a manifestation of fluid volume excess?
Which of the following is a manifestation of fluid volume excess?
What is the primary difference between diabetes insipidus and SIADH?
What is the primary difference between diabetes insipidus and SIADH?
Which of the following is NOT a potential manifestation of diabetes insipidus?
Which of the following is NOT a potential manifestation of diabetes insipidus?
What is the most likely reason why someone with SIADH may experience dilutional hyponatremia?
What is the most likely reason why someone with SIADH may experience dilutional hyponatremia?
What is a common manifestation of hyponatremia?
What is a common manifestation of hyponatremia?
Which condition is characterized by a serum sodium level of 145 mEq/L?
Which condition is characterized by a serum sodium level of 145 mEq/L?
What could occur due to hyperkalemia?
What could occur due to hyperkalemia?
What is the effect of insulin on potassium levels when blood glucose levels are very high?
What is the effect of insulin on potassium levels when blood glucose levels are very high?
What is a potential cause of hypocalcemia?
What is a potential cause of hypocalcemia?
What is indicated by a positive Chvostek sign?
What is indicated by a positive Chvostek sign?
Which electrolyte imbalance could lead to EKG changes such as a prolonged QT interval?
Which electrolyte imbalance could lead to EKG changes such as a prolonged QT interval?
What is the effect of alkalosis on calcium binding to plasma proteins?
What is the effect of alkalosis on calcium binding to plasma proteins?
Which of the following is a common manifestation of hypermagnesemia?
Which of the following is a common manifestation of hypermagnesemia?
Which condition can cause a rapid shift of potassium from ICF to ECF, leading to hyperkalemia?
Which condition can cause a rapid shift of potassium from ICF to ECF, leading to hyperkalemia?
Flashcards
Intracellular Fluid
Intracellular Fluid
Fluid within cells; rich in potassium and proteins.
Extracellular Fluid
Extracellular Fluid
Fluid outside of cells; includes interstitial and blood plasma.
Sodium Concentration Regulation
Sodium Concentration Regulation
Controlled by mechanisms like renin-angiotensin and antidiuretic hormone.
Fluid Shifts
Fluid Shifts
Signup and view all the flashcards
Electrolyte Imbalances
Electrolyte Imbalances
Signup and view all the flashcards
Dehydration
Dehydration
Signup and view all the flashcards
Syndrome of Inappropriate ADH (SIADH)
Syndrome of Inappropriate ADH (SIADH)
Signup and view all the flashcards
Diabetes insipidus
Diabetes insipidus
Signup and view all the flashcards
Osmolality
Osmolality
Signup and view all the flashcards
Isotonic solution
Isotonic solution
Signup and view all the flashcards
Hypotonic solution
Hypotonic solution
Signup and view all the flashcards
Hypertonic solution
Hypertonic solution
Signup and view all the flashcards
Capillary filtration pressure
Capillary filtration pressure
Signup and view all the flashcards
Edema
Edema
Signup and view all the flashcards
Capillary colloidal osmotic pressure
Capillary colloidal osmotic pressure
Signup and view all the flashcards
Fluid Compartments
Fluid Compartments
Signup and view all the flashcards
Extracellular Fluid (ECF)
Extracellular Fluid (ECF)
Signup and view all the flashcards
Intracellular Fluid (ICF)
Intracellular Fluid (ICF)
Signup and view all the flashcards
Electrolytes
Electrolytes
Signup and view all the flashcards
Major Cations in ECF
Major Cations in ECF
Signup and view all the flashcards
Fluid Intake Sources
Fluid Intake Sources
Signup and view all the flashcards
Fluid Distribution
Fluid Distribution
Signup and view all the flashcards
Output Regulation
Output Regulation
Signup and view all the flashcards
Hormones in Calcium Regulation
Hormones in Calcium Regulation
Signup and view all the flashcards
Histamine Release
Histamine Release
Signup and view all the flashcards
Antidiuretic Hormone (ADH)
Antidiuretic Hormone (ADH)
Signup and view all the flashcards
Sodium Balance Regulation
Sodium Balance Regulation
Signup and view all the flashcards
Thirst Mechanisms
Thirst Mechanisms
Signup and view all the flashcards
Intracellular thirst
Intracellular thirst
Signup and view all the flashcards
Fluid Volume Excess
Fluid Volume Excess
Signup and view all the flashcards
Hyponatremia
Hyponatremia
Signup and view all the flashcards
Hypernatremia
Hypernatremia
Signup and view all the flashcards
Potassium Regulation
Potassium Regulation
Signup and view all the flashcards
Hypokalemia
Hypokalemia
Signup and view all the flashcards
Hyperkalemia
Hyperkalemia
Signup and view all the flashcards
EKG Changes in Hypokalemia
EKG Changes in Hypokalemia
Signup and view all the flashcards
Calcium Forms in Blood
Calcium Forms in Blood
Signup and view all the flashcards
Hypocalcemia
Hypocalcemia
Signup and view all the flashcards
Tetany Signs
Tetany Signs
Signup and view all the flashcards
Magnesium Imbalances
Magnesium Imbalances
Signup and view all the flashcards
Study Notes
Fluid & Electrolyte Balance
- Lecture was given by Laura Madden, PhD, RN for NURS 3011
Lesson Outcomes
- Differentiate intracellular from extracellular fluid compartments in terms of water, electrolyte, and osmotically active solute distribution.
- Describe the functions and physiologic mechanisms controlling water levels and sodium concentration. This includes effective circulating volume, sympathetic nervous system, renin-angiotensin-aldosterone system, and antidiuretic hormone.
- Describe factors controlling fluid shifts between vascular and interstitial fluid compartments, and how these fluid shifts relate to edema and third spacing.
- Differentiate the pathophysiology and manifestations of diabetes insipidus, syndrome of inappropriate antidiuretic hormone, fluid volume excess/deficit, hyponatremia, and hypernatremia.
- Compare and contrast regulating factors of electrolytes, normal lab values, and the etiologies/manifestations of electrolyte imbalances related to sodium, potassium, calcium, and magnesium.
Transport Across Cell Membranes: A Review
- Cell membranes act as a barrier.
- Different types of membrane transport include:
- Simple diffusion
- Facilitated diffusion
- Primary active transport
Movement Across a Membrane and Energy
- Passive transport is easy and moves substances down a concentration gradient.
- Active transport is hard work and moves substances against a concentration gradient.
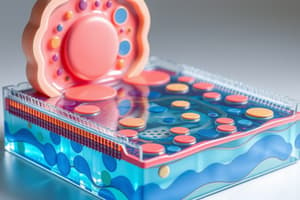
Active Transport
- This is an illustration that shows how the Na+/K+ pump works.
Fluid Compartments
- Intracellular, extracellular, and transcellular fluid
- ECF (1/3 of total body water) contains:
- Intravascular (plasma) fluid: ~20% of ECF
- Interstitial fluid: ~80% of ECF
- ICF(2/3 of total body water): inside the cells, making up ~40% of the body weight. Potassium is the major cation.
- Transcellular fluid: located in special spaces, such as the cerebrospinal fluid, pericardial fluid, peritoneal fluid, and pleural fluid, making up only ~1% of ECF.
Electrolytes
- Electrolytes are ions—charged particles.
- Cations are positively charged.
- Anions are negatively charged.
- Electrolytes maintain homeostasis by balancing cations and anions at similar concentrations in intracellular and extracellular fluids.
- Lab values are measured in mg/dL, mEq/L, or mmol/L.
Fluid and Electrolytes
- All body fluids contain electrolytes that are necessary for optimal function.
- Maintaining the balance of electrolytes and body water is dynamic and involves an interplay of processes.
Concentration of Fluid & Electrolytes
- Osmolality is the measurement of the number of dissolved solute particles in a solution.
- Normal serum osmolality is 275-295 mOsm/Kg H₂O.
- Normal urine osmolality is 500-800 mOsm/kg H₂O
Normal Physiological Processes of Fluid and Electrolytes
- Intake and absorption
- Can be administered intravenously or through other routes.
- Strongly influenced by hunger and thirst (stimulated by increased osmolality)
- Absorption or oral intake occurs in the intestines
- Distribution of ECF occurs through filtration between the two major extracellular compartments: vascular and interstitial.
- Hydrostatic pressure pushes fluid from capillaries into the interstitial space
- Colloid osmotic pressure pulls fluid from interstitial space into capillaries.
- Water moves across the semi-permeable membrane by osmosis.
- Electrolyte movement has an energy requirement.
- Output (excretion)
- Regulated physiologically via renal (urine); GI tract (feces); skin (sweat); and lungs (water vapor)
- Abnormal routes (no physiological regulatory mechanisms) include emesis, hemorrhage, drainage through tubes, etc.
Scope of Fluid & Electrolyte Balance
- Normal ECF should have optimal effective circulating volume (ECV) and electrolyte levels.
- Normal serum sodium (Na+): 135-145 mEq/L
- Normal serum osmolarity: 280-300 mOsm/kg H₂O
- Normal potassium (K+): 3.5-5.0 mEq/L
Transport of Fluid & Electrolytes
- Describes movement of fluids and electrolytes.
Renin-Angiotensin-Aldosterone System (RAAS)
- Response to decreased renal perfusion by Juxtaglomerular apparatus signals the body to increase effective circulating volume, increasing blood pressure and sodium reabsorption. This involves renin, angiotensinogen, angiotensin I, angiotensin II, and aldosterone to increase sodium reabsorption.
Antidiuretic Hormone (ADH)
- Released by the posterior pituitary gland.
- ADH alters the permeability of the collecting tubules to water, allowing more water to be absorbed.
- High ADH, causes the kidneys to reabsorb more water via the collecting ducts, producing a more concentrated urine with a higher specific gravity.
- Low ADH, causes the kidney to excrete more water via the collecting ducts, producing a less concentrated urine with a lower specific gravity
Aldosterone
- Produced and released by the adrenal cortex.
- Increases sodium and water reabsorption while increasing potassium excretion
Concentration of Fluid & Electrolytes (Conditions increasing osmolality)
- Serum: dehydration, sepsis, fever, sweating, burns, diabetes mellitus, diabetes insipidus, uremia, hypernatremia, ethanol, methanol, ethylene glycol ingestion, mannitol therapy
- Urine: dehydration, syndrome of inappropriate ADH secretion, adrenal insufficiency, glycosuria, hypernatremia, high-protein diet
Concentration of Fluid & Electrolytes (Conditions decreasing osmolality)
- Serum: excess hydration, hyponatremia, syndrome of inappropriate ADH secretion
- Urine: diabetes insipidus, excess fluid intake, acute renal insufficiency, glomerulonephritis
Capillary & Interstitial Fluid Exchange
- 4 main forces responsible for fluid transfer between capillary and interstitial spaces
- Capillary filtration pressure
- Capillary colloidal osmotic pressure
- Interstitial hydrostatic pressure
- Interstitial colloidal osmotic pressure
- Interstitial fluid increases due to increased capillary filtration pressure, decreased capillary colloidal osmotic pressure, increased capillary permeability, and obstruction of lymphatic fluid flow.
Edema
- Increased interstitial fluid volume due to:
- increased capillary filtration pressure
- decreased capillary colloidal osmotic pressure
- increased capillary permeability
- obstruction of lymphatic flow
Sodium and Water Balance
- Regulation of water balance
- Thirst
- Anti-diuretic hormone (ADH) also known as vasopressin
- Baroreceptors detect changes in blood pressure and signal pituitary
- Osmoreceptors sense diffusion of water caused by changes in serum osmolality
- Regulation of sodium balance
- Sympathetic nervous system
- Renin-Angiotensin-Aldosterone System
Thirst
- Regulated by the thirst center in the hypothalamus.
- 2 primary mechanisms:
- Extracellular thirst (decrease in blood volume)
- Intracellular thirst (increase in ECF osmolality)
- Angiotensin II (secondary)
Disorders of Fluid Balance
- Fluid Volume Excess
- Expansion of ECF compartment, usually as a result of increased total body sodium, manifests with weight gain, edema, distended neck veins, full bounding pulse, and venous distension, and pulmonary edema (severe).
- Isotonic Fluid Volume Deficit
- Loss of water and electrolytes—manifest with thirst, decreased body weight, oliguria, high urine specific gravity, dry mucous membranes, and postural hypotension, tachycardia
Disorders of Fluid Balance: ADH imbalance
- Diabetes Insipidus - Decreased secretion or response to ADH—manifests with polyuria, polydipsia, and decreased urine specific gravity.
- Syndrome of Inappropriate ADH secretion (SIADH)—Abnormal excessive secretion of ADH—manifests with decreased urinary output, dilutional hyponatremia, fluid volume overload, and increased urine specific gravity.
Syndrome of Inappropriate ADH (SIADH) Versus Diabetes Insipidus
- Compare and contrast symptoms of SIADH and Diabetes Insipidous
Sodium Imbalances - Hyponatremia
- Hyponatremia - serum sodium less than 135 mEq/L
- Types of hyponatremia
- Hypertonic hyponatremia
- Hypotonic (dilutional) hyponatremia
- Hypovolemic: loss of water and sodium due to excessive water loss.
- Euvolemic: most common—water retention (ADH)
- Hypervolemic: Failure of the body to detect hypervolemia—increased ADH
- Manifestations of hyponatremia
- Muscle cramps, weakness, headache, apprehension, stupor or coma, nausea, vomiting, and diarrhea
- Types of hyponatremia
Sodium Imbalances - Hypernatremia
- Hypernatremia - serum sodium greater than 145 mEq/L
- Etiology - net water loss or net sodium gain
- Manifestations - ECF loss, cellular dehydration, decreased skin turgor, CNS manifestations (headache, agitation, decreased reflexes, seizures, coma), CV manifestations (tachycardia, weak pulses, hypotension, vascular collapse)
Potassium Regulation
- Dietary intake
- Renal regulation of K+ (aldosterone- increases secretion)
- K+/H+ exchange
- Shifts between ICF and ECF
- Na+/K+-ATPase pump
- Insulin & beta-adrenergics- increase cellular uptake
Potassium Imbalances
- Hypokalemia- serum potassium less than 3.5 mEq/L, causes include inadequate intake, excessive loss, and redistribution
- Hyperkalemia - serum potassium greater than 5.3 mEq/L, causes include decreased excretion and rapid rate of administration.
EKG Changes with Potassium Imbalances
- Provides illustrations demonstrating EKG changes associated with Potassium Imbalances.
Calcium
- 99% found in bone; 3 forms of extra-cellular calcium
- 40% bound to plasma proteins (albumin)
- 1% decrease in albumin equates to 0.8% decrease in calcium
- pH affects binding (acidosis less binding; alkalosis more binding); 10% is complexed
- 50% is not bound and is ionized – used by cells for enzymatic functions
Calcium Imbalances
- Hypocalcemia- serum calcium less than 8.29 mg/dL
- Etiology—renal failure, hypoparathyroidism, various medications
- Manifestations—positive Chvostek sign, tetany, hypotension, prolonged QT interval
- Hypercalcemia- serum calcium greater than 10.5 mg/dL
- Etiology—increased bone resorption, neoplasms, hyperparathyroidism
- Manifestations—crisis, polyuria, excessive thirst, volume deficit, fever, altered LOC, azotemia, short QT interval, AV block
Magnesium Imbalances
- Hypomagnesemia - serum magnesium <1.3 mg/dL
- Etiology - insufficient intake, increased loss
- Manifestations - tetany, tachycardia, hypertension, arrhythmias
- Hypermagnesemia - serum magnesium > 2.2 mg/dL
- Etiology - renal insufficiency
- Manifestations - hyporeflexia, hypotension, cardiac arrest
Phosphorus Imbalances
- Hypophosphatemia -
- Etiology - respiratory alkalosis, hyperglycemia, Vitamin D deficiency, chronic diarrhea, inadequate phosphate in diet, various issues affecting bone or blood.
- Manifestations - weakness, CNS dysfunction, hypotension, cardiac failure, various hematologic disorders.
- Hyperphosphatemia - -Etiology - renal insufficiency, hypoparathyroidism, respiratory acidosis, cow's milk. -Manifestations - hypocalcemia, oliguria, poor appetite, calcifications in organs.
Key Things to Remember About Electrolytes
- Sodium (Na+)
- Potassium (K+)
- Calcium (Ca+)
- Magnesium (Mg+)
Studying That Suits You
Use AI to generate personalized quizzes and flashcards to suit your learning preferences.