Podcast
Questions and Answers
What is the normal range of creatinine levels in women?
What is the normal range of creatinine levels in women?
- 0.5-1.5 mg/dL
- 0.7-1.3 mg/dL
- 0.6-1.1 mg/dL (correct)
- 1.0-1.5 mg/dL
What is the primary function of erythropoietin?
What is the primary function of erythropoietin?
- To produce active form of vitamin D
- To stimulate aldosterone production
- To regulate hematocrit (correct)
- To regulate blood pressure
What is the result of damage to all four components of the nephron?
What is the result of damage to all four components of the nephron?
- Renal disease
- Glomerular filtration rate decrease
- Renal failure
- End-stage renal disease (correct)
What is the function of the glomerular basement membrane?
What is the function of the glomerular basement membrane?
What is the primary function of the α 1 hydroxylase enzyme?
What is the primary function of the α 1 hydroxylase enzyme?
What is the glomerular filtration rate (GFR) for renal disease?
What is the glomerular filtration rate (GFR) for renal disease?
What is the function of the mesangial cells?
What is the function of the mesangial cells?
What is the normal range of blood urea nitrogen (BUN) levels?
What is the normal range of blood urea nitrogen (BUN) levels?
What is the primary function of nephrin in the glomerular basement membrane?
What is the primary function of nephrin in the glomerular basement membrane?
What is the underlying mechanism of circulating immune complex nephritis?
What is the underlying mechanism of circulating immune complex nephritis?
What is the effect of abnormalities in nephrin on the glomerular basement membrane?
What is the effect of abnormalities in nephrin on the glomerular basement membrane?
What is the primary mechanism of injury in antibody-associated glomerulonephritis?
What is the primary mechanism of injury in antibody-associated glomerulonephritis?
What is the role of macrophages in immune complex nephritis?
What is the role of macrophages in immune complex nephritis?
What is the primary site of immune complex deposition in circulating immune complex nephritis?
What is the primary site of immune complex deposition in circulating immune complex nephritis?
What is the primary function of disulfide bridges in nephrin?
What is the primary function of disulfide bridges in nephrin?
What is the primary characteristic of immune complex nephritis?
What is the primary characteristic of immune complex nephritis?
What is the characteristic immunofluorescence pattern in membranous nephropathy?
What is the characteristic immunofluorescence pattern in membranous nephropathy?
What is the most common cause of nephrotic syndrome in children?
What is the most common cause of nephrotic syndrome in children?
What is the primary cause of nephrotic syndrome in adults?
What is the primary cause of nephrotic syndrome in adults?
What is the characteristic pathology finding in minimal-change nephropathy?
What is the characteristic pathology finding in minimal-change nephropathy?
What is the response to steroid therapy in membranous nephropathy?
What is the response to steroid therapy in membranous nephropathy?
What is the characteristic clinical presentation of nephrotic syndrome?
What is the characteristic clinical presentation of nephrotic syndrome?
What is the primary cause of focal segmental glomerulosclerosis?
What is the primary cause of focal segmental glomerulosclerosis?
What is the prognosis of focal segmental glomerulosclerosis?
What is the prognosis of focal segmental glomerulosclerosis?
What is the characteristic pathology finding in membranous nephropathy?
What is the characteristic pathology finding in membranous nephropathy?
What is the age range affected by minimal-change nephropathy?
What is the age range affected by minimal-change nephropathy?
Which of the following is a characteristic of nephritic syndrome?
Which of the following is a characteristic of nephritic syndrome?
What is the primary mechanism of injury in Goodpasture syndrome?
What is the primary mechanism of injury in Goodpasture syndrome?
Which of the following is a typical finding in rapidly progressive glomerulonephritis?
Which of the following is a typical finding in rapidly progressive glomerulonephritis?
What is the primary treatment for Goodpasture syndrome?
What is the primary treatment for Goodpasture syndrome?
Which of the following is a characteristic of mixed nephritic/nephrotic syndrome?
Which of the following is a characteristic of mixed nephritic/nephrotic syndrome?
What is the primary mechanism of injury in rapidly progressive glomerulonephritis?
What is the primary mechanism of injury in rapidly progressive glomerulonephritis?
Which of the following is a characteristic of nephrotic syndrome?
Which of the following is a characteristic of nephrotic syndrome?
What is the primary site of injury in Goodpasture syndrome?
What is the primary site of injury in Goodpasture syndrome?
What is the primary mechanism of injury in nephritic syndrome?
What is the primary mechanism of injury in nephritic syndrome?
What is the function of the lower urinary tract?
What is the function of the lower urinary tract?
What is the most common route of bacterial infection in the urinary tract?
What is the most common route of bacterial infection in the urinary tract?
What is pyelonephritis?
What is pyelonephritis?
What is the most common cause of pyelonephritis?
What is the most common cause of pyelonephritis?
What is acute pyelonephritis?
What is acute pyelonephritis?
What is a common complication of urinary tract infections?
What is a common complication of urinary tract infections?
What is a possible route of bacterial infection in the urinary tract?
What is a possible route of bacterial infection in the urinary tract?
What is a common cause of pyelonephritis?
What is a common cause of pyelonephritis?
What is the epithelial lining of the urinary tract?
What is the epithelial lining of the urinary tract?
What is a group of disorders that affect the lower urinary tract?
What is a group of disorders that affect the lower urinary tract?
What is the main cause of chronic pyelonephritis?
What is the main cause of chronic pyelonephritis?
What is the result of vesicoureteral reflux?
What is the result of vesicoureteral reflux?
What is the most common cause of acute tubular injury?
What is the most common cause of acute tubular injury?
What is the typical clinical presentation of acute tubular injury?
What is the typical clinical presentation of acute tubular injury?
What is the cause of reflux nephropathy?
What is the cause of reflux nephropathy?
What is the typical finding in tubulointerstitial nephritis?
What is the typical finding in tubulointerstitial nephritis?
What is the common form of chronic pyelonephritis?
What is the common form of chronic pyelonephritis?
What is the outcome of acute tubular injury determined by?
What is the outcome of acute tubular injury determined by?
What is the result of damage to the tubules and interstitium?
What is the result of damage to the tubules and interstitium?
What is the characteristic of benign nephrosclerosis?
What is the characteristic of benign nephrosclerosis?
What is the histopathological feature of benign nephrosclerosis?
What is the histopathological feature of benign nephrosclerosis?
What is the age group commonly affected by benign nephrosclerosis?
What is the age group commonly affected by benign nephrosclerosis?
What is the difference between benign and malignant nephrosclerosis?
What is the difference between benign and malignant nephrosclerosis?
What is the underlying cause of nephrosclerosis?
What is the underlying cause of nephrosclerosis?
What is the characteristic kidney texture in nephrosclerosis?
What is the characteristic kidney texture in nephrosclerosis?
What is the association between nephrosclerosis and diabetes mellitus?
What is the association between nephrosclerosis and diabetes mellitus?
What is the difference between nephrosclerosis and arteriosclerosis?
What is the difference between nephrosclerosis and arteriosclerosis?
What is the clinical presentation of benign nephrosclerosis?
What is the clinical presentation of benign nephrosclerosis?
What is the primary characteristic of Malignant Nephrosclerosis?
What is the primary characteristic of Malignant Nephrosclerosis?
What is the underlying mechanism of Diabetic Renal Disease?
What is the underlying mechanism of Diabetic Renal Disease?
What is the characteristic pathology finding in Chronic Kidney Disease?
What is the characteristic pathology finding in Chronic Kidney Disease?
Which of the following is a characteristic of autosomal dominant polycystic kidney disease?
Which of the following is a characteristic of autosomal dominant polycystic kidney disease?
What is the primary cause of death in polycystic kidney disease?
What is the primary cause of death in polycystic kidney disease?
What is the primary complication of Diabetic Renal Disease?
What is the primary complication of Diabetic Renal Disease?
What is the genetic mutation associated with autosomal recessive polycystic kidney disease?
What is the genetic mutation associated with autosomal recessive polycystic kidney disease?
What is the characteristic clinical presentation of Malignant Nephrosclerosis?
What is the characteristic clinical presentation of Malignant Nephrosclerosis?
What is the primary treatment for end-stage renal disease?
What is the primary treatment for end-stage renal disease?
What is the characteristic clinical presentation of polycystic kidney disease?
What is the characteristic clinical presentation of polycystic kidney disease?
What is the primary mechanism of chronic renal failure from Diabetic Renal Disease?
What is the primary mechanism of chronic renal failure from Diabetic Renal Disease?
What is the primary complication of polycystic kidney disease?
What is the primary complication of polycystic kidney disease?
What is the age range affected by autosomal dominant polycystic kidney disease?
What is the age range affected by autosomal dominant polycystic kidney disease?
What is the primary cause of urinary calculi formation?
What is the primary cause of urinary calculi formation?
Which of the following is NOT a common location for urinary calculi formation?
Which of the following is NOT a common location for urinary calculi formation?
What is the most common type of urinary calculi?
What is the most common type of urinary calculi?
What is the primary reason for the association of idiopathic hypercalciuria with calcium oxalate stones?
What is the primary reason for the association of idiopathic hypercalciuria with calcium oxalate stones?
What is the percentage of calcium oxalate stones associated with idiopathic hypercalciuria?
What is the percentage of calcium oxalate stones associated with idiopathic hypercalciuria?
What is the primary symptom of urinary calculi?
What is the primary symptom of urinary calculi?
What is the primary complication of urinary calculi?
What is the primary complication of urinary calculi?
What is the primary mechanism of stone formation in urinary calculi?
What is the primary mechanism of stone formation in urinary calculi?
What is the primary location for struvite stone formation?
What is the primary location for struvite stone formation?
What is the primary mechanism of stone formation in Struvite calculi?
What is the primary mechanism of stone formation in Struvite calculi?
What is the characteristic of Wilms tumor in children?
What is the characteristic of Wilms tumor in children?
What is the primary risk factor for renal cell carcinoma?
What is the primary risk factor for renal cell carcinoma?
What is the characteristic of clear cell renal carcinoma?
What is the characteristic of clear cell renal carcinoma?
What is the primary complication of hydronephrosis?
What is the primary complication of hydronephrosis?
What is the primary association of Beckwith-Wiedemann syndrome?
What is the primary association of Beckwith-Wiedemann syndrome?
What is the primary characteristic of Staghorn calculi?
What is the primary characteristic of Staghorn calculi?
What is the primary mechanism of injury in hydronephrosis?
What is the primary mechanism of injury in hydronephrosis?
What is the primary association of von Hippel-Landau disease?
What is the primary association of von Hippel-Landau disease?
What is the primary characteristic of uric acid stones?
What is the primary characteristic of uric acid stones?
Flashcards are hidden until you start studying
Study Notes
Kidney Functions
- Regulate blood pressure
- Maintain ion balance by absorbing water and salts to regulate concentration in plasma
- Secrete hormones, including erythropoietin for producing red blood cells and regulating hematocrit
- Produce enzyme α 1 hydroxylase to produce active form of vitamin D
- Excrete soluble waste products in the form of urine
- Regulate renin, which activates angiotensin, constricting peripheral vessels and stimulating aldosterone
- Aldosterone acts on tubules to reabsorb sodium ions and water, maintaining plasma volume and normal blood pressure
Laboratory Values for Kidney Function
- Normal levels: Blood urea nitrogen (BUN) 6-20 mg/dL, Creatinine based on size and muscle mass (Men 0.7-1.3 mg/dL, Women 0.6-1.1 mg/dL)
- Glomerular filtration rate (GFR) ages 40 and below: Men 100-130 mL/min, Women 90-120 mL/min, decreases after 40 years of age
- GFR for renal disease: under 60 mL/min, GFR for renal failure: under 15 mL/min
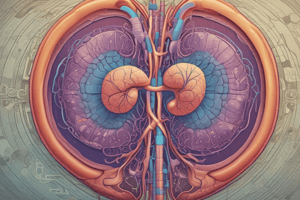
Nephron
- Functional unit of the kidney, divided into four components: Glomerulus, Tubule, Interstitium, and Blood vessels
- Damage to all four components results in end-stage renal disease
- Glomerulus filters, Tubule reabsorbs, Interstitium supports, and Blood vessels deliver arterial blood and return venous blood
Glomerulus
- Anastomosing network of capillaries invested by two layers of epithelium: Visceral epithelium and Parietal epithelium
- Visceral epithelium: Made of podocytes, becomes part of the capillary wall, critical to maintenance of glomerular barrier function, diffusion barrier to proteins, and responsible for synthesis of glomerular basement membrane components
- Parietal epithelium: Lines Bowman space where plasma filtrate is collected first, continuous with tubular epithelium
Glomerular Capillary Wall
- Filtering mechanism consists of fenestrated endothelial cells, glomerular basement membrane, and visceral epithelial cells (podocytes)
- Podocytes possess foot processes bridged by thin slit diaphragm
- Basement membrane made of Type IV collagen, prevents large molecules and anionic proteins into Bowman space
- Mesangial tuft-supported by mesangial cells found in between capillaries, can contract, proliferate, lay down collagen and other matrix components, and promote leukocyte recruitment and growth factors to support glomerular tuft
Glomerular Filtration
- Permeable to water, small solutes, and solutes that are cationic
- Impermeable to molecules with size and charge of albumin (large and anionic)
Nephrin and Glomerular Function
- Nephrin is a major component of slit diaphragms between adjacent foot processes, bound together by disulfide bridges.
- It plays a critical role in selective permeability of the glomerular basement membrane.
- Abnormalities in nephrin allow abnormal leakage of plasma proteins, leading to nephrotic syndrome.
Glomerular Diseases
- The most common cause of primary glomerulopathy is immune mechanisms, involving glomerular deposits of immunoglobulins and a Type III hypersensitivity reaction.
- The antigen is not of glomerular origin, and can be endogenous (e.g. systemic lupus erythematosus) or exogenous (e.g. bacterial, viral).
- Circulating immune complexes can cause injury, leading to activation of complement and leukocyte infiltration.
Forms of Antibody-Associated Injury
- There are two forms of antibody-associated injury:
- In-situ antibody reaction within the glomerulus, resulting in granular deposition on immunofluorescence (e.g. membranous nephropathy).
- Deposition of circulating antigen-antibody complex, resulting in linear deposition on immunofluorescence.
Nephrotic Syndrome
- Nephrotic syndrome is caused by derangement in capillary walls of the glomerulus, leading to structural changes or alterations in the glomerular basement membrane or mesangium.
- Clinical presentation includes proteinuria, hypoalbuminemia, generalized edema, lipiduria, and hyperlipidemia.
- In all cases of nephrotic syndrome, there is fusion of epithelial foot processes.
- If affecting children, the lesion is primary to the kidney, while if affecting adults, it is related to systemic diseases (e.g. diabetes, amyloidosis, systemic lupus).
Primary Causes of Nephrotic Syndrome
- Primary causes include:
- Minimal-change nephropathy
- Membranous nephropathy
- Focal segmental glomerulosclerosis
Secondary Causes of Nephrotic Syndrome
- Secondary causes include:
- Diabetes mellitus
- Lupus erythematosus
- Amyloidosis
- Infections (e.g. Hepatitis B, HIV, Malaria, Syphilis)
- Preeclampsia
Minimal Change Nephropathy
- Minimal change nephropathy is the most frequent cause of nephrotic syndrome in children.
- It is idiopathic and affects ages 1 to 7.
- Pathology is detected only with electron microscopy, and loss or damage of foot processes (podocyte) is seen.
- It responds well to steroids, but recurrence occurs in more than two-thirds of cases.
Membranous Nephropathy
- Membranous nephropathy is a form of chronic immune-complex mediated disease.
- It is slowly progressive and affects ages 30-60.
- Primary variant is an autoimmune condition, while secondary variant is associated with infections, systemic lupus, exposure to gold or mercury, cancers, and drugs.
- Subepithelial immunoglobulin deposits along the glomerular basement membrane are seen, leading to diffuse thickening of the capillary wall.
Focal Segmental Glomerulosclerosis
- Focal segmental glomerulosclerosis is the most common cause of nephrotic syndrome in adults.
- It is a primary disorder of podocytes (epithelial injury) and affects focal areas and segments of glomeruli.
- It can be primary (idiopathic) or secondary, and is associated with HIV, heroin addiction, response to nephron loss, and severe obesity or chronic kidney disease.
- It can affect children and can progress to end-stage kidney disease within 10 years of diagnosis.
Nephrin and Glomerular Function
- Nephrin is a major component of slit diaphragms between adjacent foot processes, bound together by disulfide bridges.
- It plays a critical role in selective permeability of the glomerular basement membrane.
- Abnormalities in nephrin allow abnormal leakage of plasma proteins, leading to nephrotic syndrome.
Glomerular Diseases
- The most common cause of primary glomerulopathy is immune mechanisms, involving glomerular deposits of immunoglobulins and a Type III hypersensitivity reaction.
- The antigen is not of glomerular origin, and can be endogenous (e.g. systemic lupus erythematosus) or exogenous (e.g. bacterial, viral).
- Circulating immune complexes can cause injury, leading to activation of complement and leukocyte infiltration.
Forms of Antibody-Associated Injury
- There are two forms of antibody-associated injury:
- In-situ antibody reaction within the glomerulus, resulting in granular deposition on immunofluorescence (e.g. membranous nephropathy).
- Deposition of circulating antigen-antibody complex, resulting in linear deposition on immunofluorescence.
Nephrotic Syndrome
- Nephrotic syndrome is caused by derangement in capillary walls of the glomerulus, leading to structural changes or alterations in the glomerular basement membrane or mesangium.
- Clinical presentation includes proteinuria, hypoalbuminemia, generalized edema, lipiduria, and hyperlipidemia.
- In all cases of nephrotic syndrome, there is fusion of epithelial foot processes.
- If affecting children, the lesion is primary to the kidney, while if affecting adults, it is related to systemic diseases (e.g. diabetes, amyloidosis, systemic lupus).
Primary Causes of Nephrotic Syndrome
- Primary causes include:
- Minimal-change nephropathy
- Membranous nephropathy
- Focal segmental glomerulosclerosis
Secondary Causes of Nephrotic Syndrome
- Secondary causes include:
- Diabetes mellitus
- Lupus erythematosus
- Amyloidosis
- Infections (e.g. Hepatitis B, HIV, Malaria, Syphilis)
- Preeclampsia
Minimal Change Nephropathy
- Minimal change nephropathy is the most frequent cause of nephrotic syndrome in children.
- It is idiopathic and affects ages 1 to 7.
- Pathology is detected only with electron microscopy, and loss or damage of foot processes (podocyte) is seen.
- It responds well to steroids, but recurrence occurs in more than two-thirds of cases.
Membranous Nephropathy
- Membranous nephropathy is a form of chronic immune-complex mediated disease.
- It is slowly progressive and affects ages 30-60.
- Primary variant is an autoimmune condition, while secondary variant is associated with infections, systemic lupus, exposure to gold or mercury, cancers, and drugs.
- Subepithelial immunoglobulin deposits along the glomerular basement membrane are seen, leading to diffuse thickening of the capillary wall.
Focal Segmental Glomerulosclerosis
- Focal segmental glomerulosclerosis is the most common cause of nephrotic syndrome in adults.
- It is a primary disorder of podocytes (epithelial injury) and affects focal areas and segments of glomeruli.
- It can be primary (idiopathic) or secondary, and is associated with HIV, heroin addiction, response to nephron loss, and severe obesity or chronic kidney disease.
- It can affect children and can progress to end-stage kidney disease within 10 years of diagnosis.
Nephritic Syndrome
- Characterized by acute onset and immunologically mediated glomerular injury
- Clinical presentation includes:
- Hematuria
- Azotemia (increase in blood urea nitrogen and serum creatinine levels)
- Oliguria
- Hypertension
- Proteinuria (less than in nephrotic syndrome)
- Pathogenesis involves:
- Proliferation of cells within glomerulus
- Leukocytic infiltration
- Injury to capillary walls, leading to red blood cells in urine
- Reduced glomerular filtration rate (GFR) and glomerular inflammation
Rapidly Progressive Glomerulonephritis (Crescentic Glomerulonephritis)
- Clinical syndrome characterized by:
- Rapid loss of renal function (acute renal failure)
- Typical findings of nephritic syndrome, including severe oliguria
- Presence of crescent-shaped epithelial cells in Bowman capsule
- Can be immune-mediated or idiopathic
- Characterized by breaks in glomerular basement membrane, leading to leakage of blood proteins
- If untreated, leads to renal failure within weeks to months
- Treated with immunosuppressive drugs
Goodpasture Syndrome (Disease)
- Autoimmune disease affecting both lungs and kidneys simultaneously
- Example of Type II hypersensitivity and rapidly progressive glomerulonephritis
- Antibodies directed against fixed antigens in glomerular basement membrane and cross-react with basement membrane of lung alveoli (antibodies against collagen IV)
- Antibodies have a linear pattern on immunofluorescence
- Treated with plasmapheresis
Summary of Glomerular Diseases
- Nephrotic syndrome:
- Abnormal loss of protein in urine
- Structural change in glomerular basement membrane or excessive mesangial matrix
- Nephritic syndrome:
- Blood in urine (hematuria)
- Glomerular damage with proliferation of endothelial or mesangial cells
- Mixed nephritic/nephrotic syndrome (seen in lupus):
- Damage to basement membrane and cell proliferation
- Rapid damage to glomerulus can lead to acute renal failure
Lower Urinary Tract
- Extends from calyces in the kidneys to the distal end of the urethra
- Transmits urine from the kidney to the exterior with the bladder as a reservoir
- Lined by transitional epithelium (urothelium)
- Five groups of disorders:
- Infection
- Obstruction
- Urinary calculi (kidney stones)
- Tumors
- Congenital diseases
Routes of Infection
- Two routes for bacteria to reach the kidney:
- Hematogenous (bloodstream)
- Seen in the elderly
- Examples: infective bacterial endocarditis, sepsis
- Ascending
- Most common
- Involves the lower urinary tract
- Common cause of pyelonephritis
- Hematogenous (bloodstream)
Pyelonephritis
- Common disease of the kidney
- Inflammation affects tubules, interstitium, and renal pelvis
- Serious complication of urinary tract infection
- Affects the bladder (cystitis), kidneys, and collecting systems
- Can be acute or chronic
Acute Pyelonephritis
- Caused by bacterial infection
- Associated with urinary tract infection (85% caused by gram-negative bacteria, E. coli)
- Complications:
- Papillary necrosis (especially in diabetics, sickle cell anemia, and urinary tract obstruction)
- Pyonephrosis (pus not draining and filling the pelvis)
- Perinephric abscess
- Symptoms:
- Chills, fever, nausea, and malaise (signs of infection)
- Pain at the costovertebral angle
- Urinary tract infection symptoms (dysuria, frequency, and urgency)
Chronic Pyelonephritis
- Known cause of chronic kidney disease
- Caused by bacterial infection, vesicoureteral reflux, obstruction, and repeat episodes of acute pyelonephritis
- Causes scarring of calyces and pelvis
- Hypertension may be a presenting symptom
- Two forms:
- Chronic obstructive
- Reflux nephropathy
Chronic Pyelonephritis
- Chronic obstructive:
- Result of recurrent infection
- Can be unilateral or bilateral
- Reflux nephropathy:
- Common form
- Occurs in childhood
- Results from kidney stones or unilateral obstruction to the ureter
- Can be unilateral or bilateral
Vesicoureteral Reflux
- Results from congenital absence or shortening of the ureter
- Valve is incompetent (does not close properly, allowing backflow of urine into the bladder)
- Reflux of bladder urine into ureters
- Ascending infection occurs
- Present in 20-40% of children with urinary tract infection
- Can result from spinal cord injury, bladder dysfunction secondary to diabetes in adults
Tubulointerstitial Nephritis
- Inflammation of tubules and interstitium
- Non-bacterial in origin
- Can be acute or chronic
- Can be caused by immune reaction to:
- Drugs
- Radiation
- Systemic autoimmune disorders
- Drugs include:
- Penicillins (ampicillin)
- Rifampin
- Diuretics (furosemide)
- Proton-pump inhibitors (omeprazole)
- NSAIDs
- Drug reaction can be:
- Type I reaction
- Type IV reaction
- Removal of the drug, normal renal function can return in several months
- Clinical presentation due to drug reaction:
- Hematuria
- Proteinuria (may be present, could be minimal)
- White cells, including eosinophils
- Fever, eosinophilia, and rash (15-25%)
Acute Tubular Injury (Acute Tubular Necrosis)
- Damage to tubular epithelial cells and reduced blood flow
- Most common cause of acute renal injury (was known as acute renal failure)
- Reversible
- Two forms:
- Ischemic
- Nephrotoxic (Direct toxic injury)
Acute Tubular Injury (Acute Tubular Necrosis)
- Ischemic:
- Most common
- Inadequate blood flow (generalized or localized reduction)
- Results from:
- Shock
- Mismatched blood transfusions
- Hemolytic processes
- Affects epithelial cells of straight portions of proximal tubules and ascending limbs
- Nephrotoxic (Direct toxic injury):
- Cause injury to proximal tubules
- Caused by:
- Poisons
- Heavy metals (mercury)
- Organic chemicals
- Drugs (gentamicin)
- Contrasting agents
- Clinical manifestations of Ischemic ATI:
- Electrolyte abnormalities
- Acidosis
- Uremia (clinical signs and symptoms of severe form of azotemia)
- Decreased GFR/Increased serum creatinine
- Oliguria/Anuria
- Outcome determined by duration and extent of injury
Diseases of Blood Vessels
- Diseases of kidneys involve vasculature secondarily
- Nephrosclerosis: sclerosis of renal arterioles and small arteries
- Associated with hypertension
- Kidney may have granular texture
Benign Nephrosclerosis
- Associated with hypertension and diabetes mellitus
- Slow progressive rise in blood pressure
- Usually identified at autopsy in people over age 60
- Presents as hyaline arteriolosclerosis
- Vessel walls thickened
- Decreased blood flow results in ischemia and diffuse tubular atrophy
Malignant Nephrosclerosis
- True medical emergency
- Can arise without pre-existing hypertension
- Characterized by:
- Papilledema
- Encephalopathy
- Cardiovascular abnormalities
- Ischemic damage (activates renin-angiotensin system)
- Fibrinoid necrosis of arterioles and small arteries
ALIG (Atheroembolic Renal Disease)
- Most common cause of end-stage renal disease
- Complications:
- Renal ischemia-atherosclerosis in large, medium, small arteries
- Glomerular damage-hyaline arteriosclerosis in efferent arterioles
- Susceptible to bacterial infection (acute pyelonephritis) and papillary necrosis
- Glomerular damage:
- Diffuse thickening of glomerular capillary basement membrane
- "Fibrin caps" on surface of glomerulus
- Kimmelstiel-Wilson nodules
- Chronic renal failure results from hyalinization of glomerulus with obliterated capillary loops and death of individual nephrons
Diabetic Renal Disease
- Necrotic papillae (papillary necrosis)
- Tips of papillae undergo necrosis
- Shed in urine and cause acute renal failure
- Caused by inflammatory thrombosis in vasa recta supplying renal papillae
- Associated with:
- Acute pyelonephritis
- Obstructive uropathy
- Analgesic nephropathy
- Bacterial infection
- Reduced neutrophil function
- Will have granular texture to kidneys
Chronic Kidney Disease
- Severe renal disease
- Progressive loss of nephrons
- Extensive scarring of glomeruli
- Usually asymptomatic, discovered late in course
- Electrolyte disturbances
- Hypertension can cause rapid decline in function
- Adaptive mechanisms:
- Hyperfiltration by remaining glomeruli
- Hemodynamic changes can lead to more damage
- Diagnosed by routine medical exam:
- Proteinuria
- Hypertension
- Azotemia
- Can die from uremia
- Treatment includes dialysis or renal transplant
Polycystic Disease
- Can be hereditary, developmental, or acquired
- Found on chromosomes 4 (PKD-2) and 16 (PKD-1)
- PKD-1 found in 85-90% of cases
- PKD-2 found in 10-15% of cases
- Multiple expanding cysts
- Clinical signs and symptoms:
- Flank pain
- Hematuria
- Hypertension
- Urinary tract infections
- Can result in chronic renal failure
Autosomal Dominant Variant (Adult Polycystic)
- Affects both kidneys
- Have renal function until 4th or 5th decade
- Symptoms occur in 4th decade
- Causes renal failure (will need dialysis or transplant)
- May have saccular aneurysms, mitral valve prolapse, liver cysts
Autosomal Recessive Variant (Childhood)
- Rare
- Four subcategories: Perinatal, Neonatal, Infantile, Juvenile
- Depend on age and presence of liver lesions
- Mutation on PKHD1 gene
- Can die from liver/kidney failure
- If survive, develop liver cirrhosis
Urinary Calculi (Urolithiasis)
- Form anywhere in the urinary collecting system, resulting from increased urinary concentration that exceeds solubility
- Common locations include renal pelvis, calyces, bladder
- Male predilection
- Factors for formation:
- Increased concentration of stone constituents
- Changes in urine pH
- Bacterial infection
- Risk factors include:
- Diet
- Dehydration
- Infection
- Genetics
- Can obstruct urine flow, cause bleeding or ulceration
- Symptoms include:
- Excruciating pain
- Flank pain
- Hematuria (visible)
- Four types of urinary calculi:
- Calcium oxalate
- Struvite (magnesium ammonium phosphate)
- Uric acid
- Cysteine
Calcium Oxalate
- Most common type (80%)
- Composed of calcium oxalate or calcium phosphate
- 55% associated with idiopathic hypercalciuria
- 5-10% caused by hypercalcemia
- Can be associated with:
- Hyperparathyroidism
- Vitamin D excess
- Sarcoidosis
Struvite (Triple Stone)
- 2nd most common type (10%)
- Composed of magnesium ammonia phosphate
- Associated with lower urinary tract infection
- Can be associated with infections of urea-splitting bacteria (Staph aureus or Proteus vulgaris)
- Can create large stones (Staghorn) in the renal pelvis and calyceal system
Uric Acid
- 6-7% of urinary calculi
- Acidic urine
- Predisposed by gout or acute leukemia
- 50% do not have hyperuricemia
- Appear radiolucent
Cystine
- 1-2% of urinary calculi
- Form due to acidic urine
Staghorn Calculi in the Pelvicalyceal System
- Can create large stones in the renal pelvis and calyceal system
Hydronephrosis
- Dilation of renal pelvis and calyces caused by obstruction of outflow of urine
- Can be sudden or gradual, congenital or acquired
- Congenital causes:
- Atresia of urethra
- Abnormal position of kidney
- Acquired causes:
- Foreign body (urolith-stone)
- Benign prostate hyperplasia
- Prostate cancer
- Bladder neoplasms
- Inflammatory lesion (prostatitis)
- Neurogenic paralysis
- Pregnancy
- Can result in atrophy of kidneys
- Can be unilateral or bilateral with complete or incomplete obstruction
- Complete obstruction: urine cannot pass
- Bilateral obstruction: below the ureters
- Unilateral obstruction: above or at ureters
- Unilateral complete or incomplete obstruction: relieve obstruction, renal function may return to normal
- Bilateral incomplete obstruction: symptoms include polyuria and nocturia, hypertension common
- Complete bilateral obstruction: oliguria or anuria, survival minimal if obstruction not relieved
Wilms Tumor (Nephroblastoma)
- Most common primary malignant renal tumor of children
- Predominantly seen in children; peak ages 2-5
- Can be associated with three congenital malformations:
- WAGR syndrome
- Beckwith-Wiedemann syndrome
- Denys-Drash syndrome
- Clinical presentation:
- Large palpable abdominal mass
- Hematuria
- Prognosis: Good
- Treatment: chemotherapy and nephrectomy (kidney removal)
Renal Cell Carcinoma
- Primary malignancy of kidney (represents 80-85% of all kidney cancers)
- Common location: cortex
- Male predilection (2:1)
- Various types:
- Clear cell renal carcinoma (most common)
- Papillary
- Chromophobe
- Clear cell variant:
- Caused by loss/inactivation of von Hippel-Lindau gene
- Can be familial or sporadic
- Associated with von Hippel-Lindau disease
- Autosomal dominant, predisposed to tumors of cerebellum and retina
- Will have multiple, bilateral clear cell carcinomas
- Histological presentation: sheets of clear cells arranged in nests with vascular stroma
- Risk factors:
- Tobacco usage
- Hypertension
- Exposure to cadmium
- Obesity
- Clinical presentation:
- Palpable abdominal mass
- Flank pain
- Painless hematuria
- Can spread by local expansion and metastasis to lung, liver, bone, oral cavity
- Can invade renal vein and travel up inferior vena cava to heart
Studying That Suits You
Use AI to generate personalized quizzes and flashcards to suit your learning preferences.